What is called childhood clubfoot?
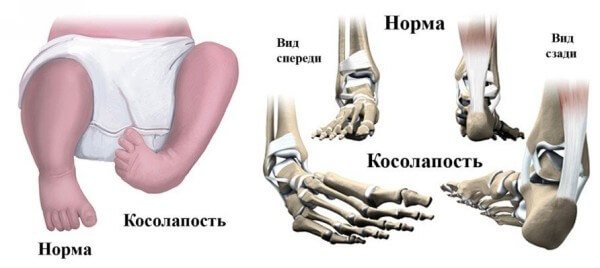
Clubfoot is a pathological condition in which a child experiences abnormal development of the ankle and foot. The development of the disease occurs due to insufficient development of muscles and ligaments, deformation of the joints of the limb.
What is the disease characterized by in newborns?
Out of 1000 babies born, only one has pathology, and often the “owners” of such a defect are male newborns. The disease is diagnosed as congenital, although in some cases clubfoot appears in children aged about 1 year. This is due to the fact that the child begins to take his first steps.
The following distinctive features are characteristic of clubfoot:
- raised heel while the foot is completely lowered;
- curled toes;
- bowed foot, often turned in an unnatural position;
- shortened foot with greater thickness;
- bent sole, on which the fold is clearly visible;
- twisted shin bones.
Clubfoot is easy to see without special instruments and devices. The pathology causes a lot of discomfort when the baby moves. He begins to limp, which inevitably leads to curvature of the spine. If a child is diagnosed with clubfoot on both limbs, this forces him to waddle in small steps.
Types of clubfoot
Foot defects are classified depending on the severity of the disease and the possibility of cure.
- Mild degree.
The deformity is not pronounced, the ankle joint retains its full mobility. You can get rid of the pathology by doing regular special gymnastics and giving your child a massage.
- Average degree.
Underdevelopment of muscles and curvature of the bone apparatus require the intervention of specialists. The pathology can be eliminated, but partially. A deformed foot will retain its shape.
- Severe degree.
The diagnosis of severe clubfoot is made in most cases in newborns. The child experiences severe limitations in movement. Radical treatment methods are used to correct the defect.
- Very severe.
This type of pathology cannot be treated, even surgically. The defect leads to disability of the child.
Risk factors
Clubfoot most often occurs in a certain group of children. The following risk factors for pathology are known:
- Gender of the child.
Boys are more often susceptible to pathological development of the foot.
- Heredity.
If in a family at least one of the parents or children has clubfoot, then with a high probability the baby carried by the mother will have the corresponding pathology.
Treatment
The principle of positive treatment of clubfoot is early contact with a specialist. The task is not only to correct the existing defect, but also to consolidate the results of the necessary therapy. Congenital clubfoot begins to be treated within a week after the baby is born, and is corrected until the child begins to walk.
A special plaster cast is applied, which is changed every week. This procedure is done until there is a visual change in the shape of the foot. After this, an individual splint is made, which is placed only at night.
You can correct clubfoot in a child using the effective Vilensky technique; a positive result is achieved much faster, within a year. Treatment involves gradual plaster casting. The doctor first stretches the leg, gradually changing its position without using force, then applies a plaster cast. Such manipulations are performed until the desired result is achieved.
Special orthopedic structures are used to fix the joints. A prerequisite is physiotherapy and kinesiotherapy. Relaxing baths, therapeutic massage, and special exercises help consolidate the results and help heal the child. After therapy, you need to wear special orthopedic shoes with a hard back.
Botox is used to treat clubfoot in children. The drug is injected into the calf muscle. When the muscle relaxes, the Achilles tendon becomes weak and the foot assumes the correct position. This technique can be used for mild clubfoot.
In severe cases of the disease or neglect and ineffectiveness of conservative treatment, surgical intervention is used. There are several methods to correct the existing defect. After preparatory therapy, an incision is made into the Achilles tendon.
The Ponseti method is performed under local anesthesia on an outpatient basis. After the wound has healed, when the leg is in the correct position, the patient is put on orthopedic shoes, which must be worn almost without taking off. Over time, braces are worn only at night.
Older children undergo surgery using the Zatsepin method - this is tendon plastic surgery. The operated leg is always smaller in size, the foot is stiffer, and periodic pain makes itself felt.
Symptoms and signs of pathology
The foot is formed before the age of 14, so starting from birth, children are susceptible to the development of pathology of the lower extremities.
Symptoms indicating clubfoot are easily noticeable:
- formation of calloused areas on the surfaces of the feet;
- painful sensations during movement;
- visible limping or bear-like walking;
- quick trampling of children's shoes.
What should parents pay attention to if their child has clubfoot?
To prevent further development of clubfoot in the baby, parents need to take action at the slightest sign of the disease. There are some nuances thanks to which adults can notice childhood pathology:
- If the child is already taking his first steps, then clubfoot can be seen by footprints in the sand or snow. A normally developed foot leaves an imprint that is located almost parallel to the other, with a slight turn outward.
- When trying to stand on your feet or move, the toes of your feet “look” inward.
Signs of clubfoot
The following signs will indicate clubfoot in children.
- When the foot is down, the heel is in a raised state.
- The inner edge of the foot is raised.
- The outer edge of the foot is drooped.
- The big toe is pointing in the wrong direction.
- You can pay attention to photos of clubfoot in children on the global network, thereby you will be able to notice other characteristic signs of this disease.
If you notice signs of clubfoot in your child, you should make an appointment with a podiatrist. Treatment of clubfoot in children, especially newborns, has a high chance of success. Quite often, a child has completely healthy feet at birth, but after a couple of years the first symptoms of clubfoot begin to appear.
Causes
Abnormal limb shape can develop under the influence of various factors. Depending on the causes of the disease, there are two forms of clubfoot: congenital and acquired.
The reason for the development of congenital foot pathology is the diagnosis of certain diseases in the mother of the child during pregnancy, as well as the exposure of the pregnant woman to bad habits:
- oligohydramnios;
- avitaminosis;
- pronounced toxicosis;
- smoking, drug use;
- incorrect position of the fetus in the last weeks of pregnancy;
- the course of viral diseases.
The acquired form of clubfoot is diagnosed in most cases in children of a small age group, but can also occur in adolescents. The reasons for the development of bone abnormalities are:
- pathological development of muscles and ligaments;
- some inflammatory diseases;
- rickets, poliomelitis, bone dysplasia;
- consuming insufficient amounts of vitamins and minerals;
- loads on the musculoskeletal system that exceed the norm;
- shoes that are the wrong size or are of poor quality;
- limb injuries of various types.
Classification of clubfoot

There are several classifications of congenital clubfoot in children. However, taking into account the latest data, it is customary to distinguish four forms of equinovarus foot deformity based on the characteristics of the cause and pathogenesis of the disease. In addition, special attention is paid to degrees of severity.
According to etiopathogenesis
The generally accepted classification is based on etiopathogenesis. Depending on the causes and mechanism of development of the defect, the following forms of congenital clubfoot in children are distinguished:
- Typical. The exact cause is unknown. It is characterized by dysplasia and persistent disruption of the location of all anatomical structures of the foot. This pathology occurs during the formation of organs and systems. There is a delay in the formation and deformation of the bones of the feet with a violation of the shape and localization of their articular surfaces. With typical congenital clubfoot, even in newborn children, it is impossible to carry out complete one-stage orthopedic correction of the foot joints.
- Positional. It is considered as an embryonic developmental disorder of the lower limb, in which shortening of the muscular-ligamentous structures in the posteromedial region of the leg and foot is observed without initial damage to the osteoarticular apparatus.
- Secondary. Develops as a result of congenital pathological changes in the neuromuscular system. Clinical symptoms directly depend on the primary disease.
- Arthrogrypotic. Occurs with severe joint pathology arthrogryposis.
By severity

Symptoms of the disease directly depend on the severity and extent of the process. The following degrees are distinguished:
- The mild form is characterized by the absence of restriction of movement in the ankle and can be corrected without significant effort.
- With moderate severity, certain restrictions of movement are observed. At the same time, when correcting the position of the foot, one feels springy compliance, but also some obstacle.
- The severe form is characterized by pronounced deformations of the osteoarticular apparatus of the foot, which in most cases cannot be corrected or corrected with manual intervention.
How to recognize pathology?
The diagnosis of congenital clubfoot is made to the child while he is in the womb. At a certain stage of pregnancy, a woman undergoes an ultrasound, which reveals childhood pathology in the development of the limbs.
After birth, the child is examined by a neonatologist. If a specialist finds symptoms of clubfoot in a newborn, he recommends that parents show the child to a doctor within a month.
When a pediatrician notices pathological changes in the limbs, he refers the adults with the small patient to a consultation with an orthopedist. At an appointment with a doctor, the probable causes of the disease are identified, and a plan for further action is developed.
The main studies prescribed by doctors to establish an accurate diagnosis and severity of the disease are:
- Radiography.
The images allow you to assess how severely the bone structure and joint have been deformed. Unfortunately, this method is not very informative for a small child due to the impossibility of obtaining a large amount of information. The bones and cartilage of a newborn are not yet fully formed, so they may not be visible in the pictures.
- Ultrasound examination of the foot.
The specialist performing the ultrasound can say with confidence how severe the changes in the soft tissues are.
- CT scan.
The study is the most informative and allows you to assess the condition of the muscular-ligamentous apparatus.
To see the overall picture of the course of the disease, the child may be prescribed general blood and urine tests.
Treatment of the disease
The method and tactics of treating the disease are determined by the form of deformation (primary, secondary), its severity, as well as the individual characteristics of the patient. The best results can be achieved by adhering to the following principles:
- early start of therapy, literally from the first days of life;
- priority of conservative methods over operational ones, but not to the point of fanaticism;
- restoration of normal support of the leg before walking;
- periodic observation of the lower extremities until the end of foot growth (for timely detection and treatment of relapses).

Methods for correcting primary congenital clubfoot
Depending on the severity of the deformity, conservative and surgical treatment methods are used.
Bandaging, massage, gymnastics for mild deformities in newborns
For mild cases of the disease, physical therapy, massage, physiotherapeutic procedures, and the application of soft bandages are used.
Considering the fact that we are mainly talking about the treatment of newborns and infants, exercise therapy is used in the form of corrective and reflex gymnastics (see below for a set of exercises for children 2-3 years old).
Principles of performing corrective gymnastics in children [2]:
- inadmissibility of pain during procedures;
- number of repetitions of exercises 8-10 times;
- number of classes – 3-4 times a day;
- warming up the lower extremities before procedures (for example, using warm baths 36-37t);
- alternating with massage techniques.
The exercises are performed in the following order: first, those aimed at eliminating adduction are used, then those that correct supination and equinus. An approximate set of corrective exercises is presented below.
- With one hand, fix the child’s foot in the ankle joint area, with the other hand, gently make straightening movements, gradually moving the forefoot outward.
- Secure the child’s left foot with the fingers of your right hand at the bottom of the lower leg and foot, and with your left hand make straightening movements, gradually moving the forefoot outward.
- Grasp the foot with the same hand, placing the thumb on the sole of the foot and the other fingers on the back side. With your other hand, grab the heel from below, firmly fixing it. Pressing your thumb upward on the outer edge of the child's foot, and downward on the inner edge of the foot (with your whole hand), lower it down.
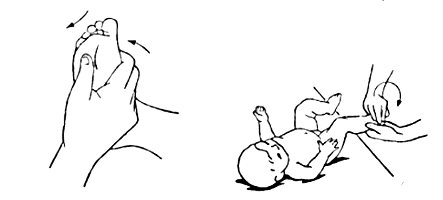
- Place the child on his stomach, bend the child's leg at the knee joint. Hold the shin with one hand and use the palm of your other hand to gently press down on your child's foot, dorsiflexing it.
- With one hand, press the child's lower leg to the table surface, fixing it in the ankle area. Another is to grab your foot so that your palm rests on the sole, and gently bend the foot dorsally while applying pressure to its outer edge. An effective combination of flexing the foot with simultaneous acupressure at the transition point of the dorsum of the foot to the lower leg.
Special massage accompanies therapeutic exercises. It includes techniques for relaxing muscles that have increased tone. These are mainly the internal and posterior muscles of the lower leg. Techniques used: stroking, shaking, vibration.
At the same time, strengthening of the stretched and weakened muscles of the front and outer parts of the lower leg is required. This is achieved by stroking them, rubbing them, kneading them [3].
In addition to special massage, general massage (arms, abdomen, back) is performed.
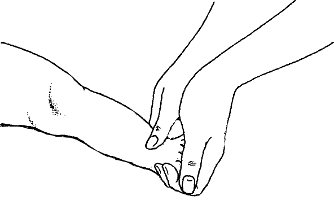
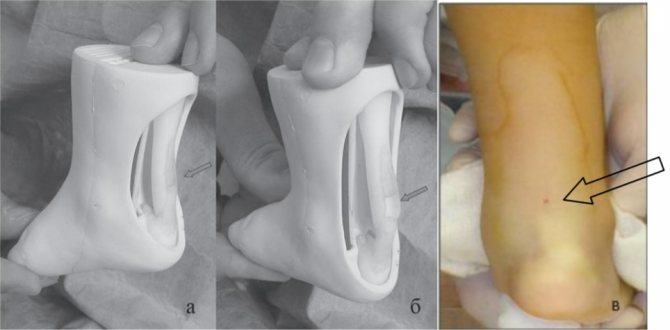
At the end of the session, the foot is placed in the position of the achieved correction and held in this position for several minutes. Afterwards, a bandage 2 m long and 5 cm wide is applied to the limb. Methods for applying a soft bandage are shown in the figure below.

Moderate degree of deformation and traditional treatment with plaster casts
In world practice, absolute preference in the treatment of any form of congenital clubfoot is given to the Ponseti method. In Russia, along with this increasingly popular method, the “old” schools of Zatsepin and Vilensky are still strong. All these methods have one thing in common - step-by-step correction of a sore foot with plaster casts . This is where the commonality between traditional methods and the Ponseti method ends.
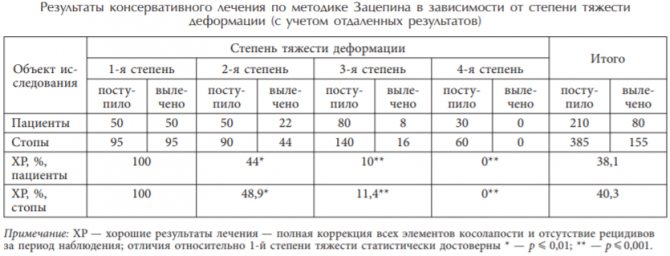
Recent studies in the field of treatment of clubfoot [12, 13, 14, 15] show the absolute unsuitability of the Zatsepin and Vilensky methods for conservative treatment of severe clubfoot. According to specialists from the Turner Institute [13, 14], the effectiveness of conservative treatment according to Zatsepin in severe forms is no more than 15%, while the effectiveness in the treatment of moderate and mild forms is 80-100%. Thus, it is advisable to limit the use of Zatsepin and Vilensky methods to the treatment of mild and moderate forms of clubfoot.
The entire period of traditional treatment can be divided into 3 stages:
- corrections;
- recording results;
- rehabilitation.
If clubfoot is diagnosed immediately after birth, then in the first 2 weeks the treatment tactics are the same as for a mild form of clubfoot. From 3-4 weeks, staged corrections with plaster casts begin to be applied. It is imperative to follow the order of correction of various parts of the foot. First, adduction and varus are corrected, then supination, and finally equinus. To eliminate each defect, up to 6 changes of dressings are required. If one of these components cannot be corrected conservatively, surgery is indicated. The volume of surgical intervention is smaller, the more corrected by casting.
Up to a year, the frequency of changing plaster casts is once a week, after 8-14 days. The procedure is performed by an orthopedic surgeon. Before plastering, a massage of the foot and lower leg is performed in combination with corrective gymnastics. After the desired position of the foot is achieved, a fenestrated circular plaster cast is applied (from the tips of the toes to the upper third of the thigh, the leg is bent at a right angle). Instead of plaster, it is possible to use special splints, but the bandage remains the tool of choice due to its ease of use, versatility, and accuracy of matching the shape of the deformed limb.
During the correction period, to prevent the development of muscle atrophy and vegetative-vascular disorders, improve trophism, and maintain the general tone of the body, it is necessary to massage the upper limbs, abdomen, and leg segments free from immobilization (including through windows in a plaster cast). In addition, electrical stimulation and electrophoresis are indicated.
Treatment with staged plaster casts according to Vilensky and Zatsepin is advisable for up to 3 years.
After eliminating foot defects, it is necessary to consolidate the result obtained. This is very important because clubfoot is a frequently recurring disease. For 3-4 months it is necessary to wear removable splints or plaster splints. They are removed only for the duration of massage, exercise therapy, and physiotherapy (warm foot baths, electrical stimulation, electrophoresis, phonophoresis, paraffin baths).
The possibilities for using exercise therapy in this period are expanding. Massage is still relevant, both general strengthening (back, abdomen, hips) and special (feet, legs). The latter is aimed at increasing the tone of the muscles of the anterior and outer surfaces of the lower leg, and at relaxing the muscles of the inner and posterior surfaces of the lower leg.
Therapeutic gymnastics is appropriate for the age of the young patient. For children under one year of age, reflex gymnastics and passive exercises are recommended (you can also use those that were indicated in the paragraph about the treatment of mild forms of clubfoot). Pronation of the foot and abduction of the forefoot are performed passively. Then the child is taught to independently hold the foot in this position. It is also recommended to flex the foot at the ankle joint in the initial positions lying on the back and on the stomach, flexion and extension of the legs at the knee and hip joints.
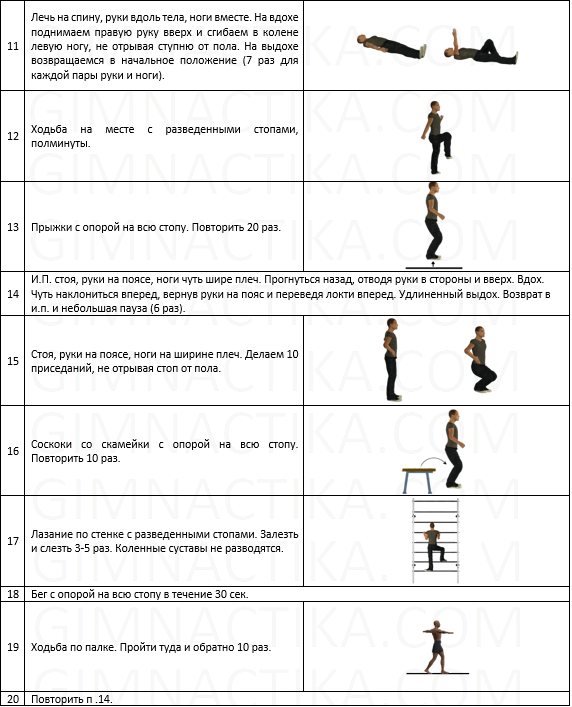
Older children are prescribed exercises with actively holding the foot in a given position. The complex of therapeutic exercises may include walking with the toe abducted outward, walking on the heels, climbing stairs with the feet apart, squats with support on the entire foot.
After removing the splints, you may be prescribed to wear splints (while you sleep) and orthopedic shoes. Physical therapy plays an important role in the rehabilitation process. Objectives of exercise therapy at the rehabilitation stage:
- consolidation of correction results and restoration of musculoskeletal function of the foot;
- fight against atrophy and contracture in joints;
- creating optimal conditions for the full growth and development of the foot;
- adaptation to increasing physical activity;
- prevention of “vicious” gait and posture disorders.
Below is an approximate set of exercises for children with congenital clubfoot.
Massage and physiotherapy also play an important role in the rehabilitation process. Swimming is very useful for the prevention and treatment of clubfoot.
Below are the results of conservative treatment according to Zatsepin, carried out until 2007 at the Federal State Budgetary Institution Research Institute for Children's Orthopedics named after. G.I. Turner [13, 14].
The use of traditional plastering is advisable up to 3 years of age.
Exercise therapy (exercises) for children aged 2 years and older
Severe form of the disease and the Ponseti method
In world practice, this method of correcting clubfoot has been used for more than 20 years, but in Russia in 2006 there were only two specialists practicing this correction method (G.M. Chochiev and M.A. Vavilov). The Ponseti method is a conservative method of treating clubfoot with elements of surgical intervention. It is also based on staged casting of the lower extremities.
Most experts believe that treatment should begin as early as possible, already at 1-2 weeks after birth. However, there are studies that call this fact into question. Thus, in work [7], in a group of patients whose treatment began a month or more after birth (but up to a year), treatment results were significantly better than those whose treatment began in the first 30 days. In addition, the authors found that foot size less than 8 cm also adversely affects the outcome of therapy.
Plaster is applied using a special technique, so treatment with the Ponseti method can only be carried out by specially trained specialists. Their list can be found on a special website. Choosing a good specialist is all the more important because the so-called “Ponsetiism” occurs, when a doctor misleads patients by saying that he treats using the Ponseti method, although in fact he uses a different technique.
The cast is applied to the limb bent at a right angle from the metatarsophalangeal joints of the fingers to the upper third of the thigh. The dressings are changed every 5-7 days [14]. As a rule, with timely treatment, 6-7 changes of plaster casts are required. This is particularly confirmed by data from a study [8], which involved 173 children with an average age of 8 months.
After achieving sufficient correction of the feet, a low-traumatic operation is performed - achillotomy (70% - 85% of patients [14]). The essence of the operation is to cut the Achilles tendon. Up to a year, surgery can be performed under local anesthesia. After the operation, a cast is applied for a month. Thus, within 2.5 months the treatment will be completed. The figure below shows the essence of achillotomy and the degree of trauma.
After removing the plaster cast, it is recommended to wear braces according to the regulations. The use of braces is an important point in treatment. Violation of the recommended bracing program leads to relapses in 80% of cases. Parents should receive comprehensive information from the attending physician about the bracing regimen and the importance of its implementation in preventing the recurrence of clubfoot during the growth of the leg and foot segment.
While wearing the braces, a restorative massage of the upper body and lower body up to the knees is indicated. Massaging the legs and feet is not recommended, as this may trigger a relapse of the disease. An exception is exercises for stretching the Achilles tendon.
The effectiveness of the Ponseti method with timely treatment (up to a year) is 95%. Also, compared to conventional casting, the duration of treatment is significantly shorter, and the age restrictions are higher (there are facts of successful correction of clubfoot even at the age of 10).
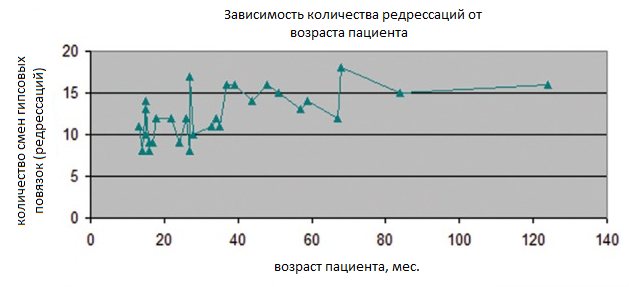
In a study [9], 30 patients aged between one and 10 years were treated with the Ponseti method. The effectiveness of therapy was 100%, although relapses of the disease were observed in 17% of cases. A direct relationship was established between the patient’s age and the number of necessary redresses (changes of plaster casts). Although age is certainly not the only factor. On average, the duration of treatment before achillotomy was 3.5 months.
A study [10] also attempted to evaluate the effectiveness of the Ponseti method for the treatment of clubfoot in late life. Data from 225 patients aged 1-16 years were analyzed. The treatment was successful in 78% of cases.
The work [10] also presents data from other studies on the treatment of uncorrected congenital clubfoot after the age of one year. The effectiveness of treatment in late age was 70-80%.
The obvious advantage of the Ponseti method over traditional casting is the ability to treat relapses. Relapses with conventional treatment often require surgical correction. After using the Ponseti method, repeated deformities can be treated in the same way (though not always). It should be noted that the most common cause of relapse is associated with incorrect wearing of braces. The Ponseti method can also be used after traditional treatment, including after surgery.
Another advantage of the Ponseti method is that there is no need to use such measures as massage, exercise therapy, physiotherapy and electrotherapy (at least not to the same extent).
The obvious disadvantages include prolonged wearing of braces (several years), which in rare cases the child may not like.
After completion of treatment, the child needs observation for up to 2–5 years for timely detection of a possible relapse of clubfoot.
Operations
Surgical treatment is usually used for severe forms of the disease or for treatment at a later age (after 3 years). There are several methods of surgical intervention:
- soft tissue operations;
- gentle operations on the foot skeleton;
- complex operations on bones.
Until the age of 12, it is advisable to perform operations only on soft tissues, but this is not always possible. Gentle operations on the foot skeleton can be performed from 4-6 years of age. Arthrodesis operations in pediatric practice are considered crippling and can only be used after 12 years of age.
Among soft tissue interventions, the Zatsepin operation has received the most recognition. The author recommends that it be performed in cases of failure of conservative treatment, relapses of clubfoot after conservative treatment, and in children with advanced forms of clubfoot after the age of 2 years. The essence of Zatsepin's operation is to lengthen the tendons along the inner and posterior surface of the ankle joint, carefully dissect the ligaments and capsule between the tibia and the bones of the foot, and intra-articular ligaments between the talus and calcaneus. After this, even a severely deformed foot is placed in the correct position. However, the relapse rate after surgery can reach 30%.
Also known are operations Sturm, Moroz, Caroll. Regardless of the type of surgical intervention, after growth has ended, patients often experience static-mechanical pain in the operated feet.
Correction of advanced forms of clubfoot using special external skeletal fixation devices is common. The most popular is the Ilizarov apparatus. Treatment based on compression-distraction devices allows for more precise relationships between the foot skeleton by stretching or compressing the bone tissue.
The Ponseti method, despite its high effectiveness even in severe cases and at a late age, also does not exclude the use of traditional surgical correction methods. In some cases, open lengthening of the Achilles tendon, posterior release of the ankle joint, relocation of the tibialis anterior tendon, etc. are required. However, all this may be required if treatment is started late, after 3 years.
Atypical clubfoot
When treating secondary congenital clubfoot, it is important not only to correct the foot deformity, but also, if possible, to eliminate the root cause of the disease. The arsenal of therapeutic agents is approximately the same as for the treatment of primary clubfoot, plus drug treatment can be added.
Considering the fact that atypical clubfoot often takes on severe, difficult to correct, highly recurrent forms, it is important to begin treatment as early as possible, from the first days of life. The works [11, 15, 16] show the possibility of using the Ponseti method for treating children with:
- arthrogryposis;
- spina bifida;
- Larsen syndrome;
- myelodysplasia;
- fibular hemimelia;
- amniotic bands.
The likelihood of subsequent surgical intervention is quite high, especially with such severe diseases as arthrogryposis.
For arthrogryposis, the treatment tactics according to Ponseti are somewhat different from those used for the idiopathic form. A larger number of plaster casts are required, an additional achillotomy may be performed before plaster casting, and braces of a different design are prescribed.
Aggravating aspects of arthrogryposis that prevent conservative correction are its generalized form, as well as the age at which treatment began. According to a study [16], 100% of feet with the distal form of the disease were treated conservatively within the age of one year. At a more mature age, the effectiveness of the Ponseti method is only 23%. With arthrogryposis multiplex, the results are even more modest.
The study [17] showed the unsuitability of traditional Vilensky casting for the treatment of arthrogrypotic clubfoot. In 100% of cases, surgical treatment was required after casting.
Acquired form of the disease
First of all, it is necessary to determine and eliminate the cause of foot deformation.
If a simple acquired form of clubfoot has been discovered, then most often fixation is carried out using special shoes, splints, massage and therapeutic exercises are prescribed. In addition, dancing and swimming are useful. If this does not help, then correction using the same Ponseti method is possible.
Paralytic clubfoot, which occurs due to damage to the peroneal nerve and muscles, or as a result of polio, is eliminated by repairing the tendons or damaged nerve. In this case, the tibialis anterior or posterior tendon is sometimes transplanted to the outside of the foot.
In case of severe deformation of the foot due to rough scars resulting from severe burns and injuries, the scars are excised and the tendons are restored. Then the patient's own tissue is transplanted.
Deformities that arise as a result of injury or osteomyelitis are eliminated by corrective osteotomies with osteoplastic surgeries. Often, an Ilizarov compression-distraction apparatus is used.
Treatment of pathology
The success of treating childhood clubfoot depends on many factors, the main ones being timely seeking medical help and receiving regular consultations with an orthopedic surgeon. The vast majority of cases of pathology are curable, with the exception of rare and particularly advanced conditions.
Depending on how severe the clubfoot is, an appropriate treatment complex is developed for the child.
Conservative methods
The method of conservative treatment of childhood clubfoot is successfully used in the early stages of the development of the pathology. To prevent surgical intervention, specialists use the following techniques:
Massage
Using massaging movements, the tone is removed from the muscular system involved in the formation of the anomaly.
Plaster "boots"
This method is the most common among others. It involves step-by-step plaster casting of a clubfoot. Before directly applying the plaster, the orthopedist carefully kneads the muscles on the child’s leg and straightens the limb so that it takes the correct position. Correction of pathology by stage-by-stage plaster casting is quite long. In some cases, treatment can last a year.
Soft bandaging
The incorrect leg is fixed with bandages. Sometimes a splint or splint is placed on the limb. The method is used only to correct mild pathology.
Vilensky's technique
The therapy allows you to eliminate clubfoot several times faster than with conventional leg casting. The technique includes a set of effective procedures: from taking baths to using orthopedic devices.
Gymnastics and exercises
Therapeutic exercises are performed daily until the desired result is achieved.
Orthotics
To correct clubfoot, orthoses are used - devices that give the foot a fixed position, close to natural.
One of the types of orthoses are splints. The child wears a rigid splint attached to the foot both during the day and during sleep.
You can learn how to cure congenital clubfoot at an early age from the video.
Medicines for illness
In the case of clubfoot treatment, medications play a secondary role. Medicines are prescribed to normalize nerve patency.
B vitamins may be prescribed as drug treatment. Botox is sometimes used. The drug is injected into the muscles, relaxing them. This helps the foot take the required position for up to 1.5 months.
Physiotherapeutic procedures
Physiotherapy is used as an auxiliary treatment for clubfoot in children over 2 years of age. Effective procedures are:
- magnetic therapy;
- electrophoresis;
- phonophoresis;
- paraffin applications for a sore joint;
- pine baths.
Carrying out surgery to correct a defect
Surgery is the very last step on the road to recovery for a child diagnosed with clubfoot. Treatment with surgery is possible in some cases:
- in case of untimely diagnosis;
- when conservative methods were not prescribed or followed;
- when diagnosing advanced stages of congenital pathology;
- with unsuccessful treatment of a child under 8 months of age.
During the operation, the ligaments and tendons of the abnormal limb are corrected. The advisability of surgical intervention is justified only when the child turns 1 year old.
Is it possible to cure clubfoot at home?
To correct clubfoot, you need to make a lot of effort to treat the pathology at home. Only mild degrees of the disease can be corrected on your own.
At home, the baby can wear special orthopedic insoles or custom-made shoes.
Great care should be taken when walking on uneven surfaces with bare feet. But this is only a small part of what is truly needed to eliminate clubfoot. The best option for your health is medical care.
The importance of orthopedic shoes
Orthopedic shoes are necessary to correct any type of clubfoot. Wearing special shoes helps the foot to form correctly and take the correct position.
Braces are used for small children. The child begins to wear them after undergoing stage-by-stage casting. With their help, the achieved result of conservative treatment is consolidated.
At the very beginning, braces are worn for 23 hours a day. Only after a few months does the orthopedist allow you to reduce the time you wear orthopedic shoes. The most famous manufacturers of specialized children's shoes are:
- Mitchells;
- Alpha Flex;
- Little bear.
It should be noted that braces are not the main method of correcting clubfoot. They are good as part of a comprehensive treatment of foot pathology.
Another unique method of treating clubfoot is described in the video.
Treatment of various forms of clubfoot in children

Many parents are seriously concerned about how to get rid of clubfoot in their child once and for all. It should be noted right away that this is not a matter of one day, week or even month. Treatment of equinovarus foot deformity requires a lot of effort, patience, time and money.
Conservative therapy
It is necessary to begin treating congenital clubfoot in children as early as possible - already from the first weeks of life. Considering the severity of the deformity and dysfunction, a set of conservative methods includes:
- retraining gymnastics (forced gradual correction of foot deformity followed by fixation with an elastic bandage);
- application of a plaster cast;
- orthopedic shoes;
- Exercise therapy with special corrective exercises;
- massage.
Gypsum bandage
In moderate and severe forms of the disease, from the age of 3 weeks they switch to the staged use of plaster casts, which are changed once every 3 weeks. At the same time, forced correction (correction) of foot deformities is carried out. The foot should be in the overcorrected position for at least 3–4 months.
The Ponseti healing method

According to the famous pediatrician Komarovsky, the Ponseti method is currently considered the optimal type of conservative treatment for congenital clubfoot in children. If you start treatment before 9 months of age, then the chances of correcting most deformities are quite high.
Treatment of clubfoot using the Ponseti method is effective in 80–90% of cases. The technique for correcting congenital clubfoot consists of 3 successive stages:
- Correction of foot deformities with plaster casts. In total, the course consists of 5–6 plasterings.
- Achillesotomy. Subcutaneous dissection of the largest tendon in humans, the Achilles tendon, to lengthen it.
- Wearing special shoes - braces to maintain the correction and prevent relapses.
Treatment is strengthened with exercise therapy, regular exercise, massage and physiotherapy.
Orthopedic shoes

For all types of acquired and congenital clubfoot in children, orthopedic shoes are used as part of the treatment and prevention of the disease. To increase efficiency, it is recommended to use orthopedic shoes together with other types of conservative treatment (physical therapy, therapeutic exercises, corrective exercises, massage, baths, fixing the foot with an elastic bandage, etc.).
According to doctor Komarovsky, parents should remember that without clear indications and prescriptions from an orthopedic doctor, purchasing and wearing special shoes is not recommended.
Using anti-varus shoes allows the baby to maintain the correct position of the foot when walking. In this case, the load on the leg is distributed extremely evenly. A distinctive feature of such shoes is the absence of instep support. In addition, children's orthopedic shoes must have laces, adjustable fasteners or Velcro to securely secure the legs.
An orthopedic doctor is obliged to teach parents how to perform special gymnastics, corrective exercises, massage and proper fixation of the foot with an elastic bandage at home.
Therapeutic gymnastics and corrective exercises
Nothing strengthens the muscular-ligamentous and osteoarticular apparatus of the lower leg and foot in case of clubfoot, like therapeutic exercises and a set of special corrective exercises. It is the responsibility of the orthopedic doctor to explain in detail and show parents all the exercises for the child that need to be performed outside of a medical institution or rehabilitation center.
Massage

Massage for clubfoot in children is an obligatory component of complex treatment for children, such as exercise therapy, gymnastics and corrective exercises.
If possible, parents should master the minimum massage skills in order to make the course of treatment continuous and increase its effectiveness.
Surgery
In severe forms of congenital clubfoot or the absence of the expected effect from conservative treatment, they proceed to surgical intervention. The main goal of surgical treatment is to eliminate existing foot deformities as much as possible.
During the rehabilitation period after surgery, it is recommended to prescribe exercise therapy with strength exercises, massage and physiotherapeutic procedures (electrophoresis, laser therapy, magnetic therapy).
Consequences of clubfoot
If you do not seek medical help in a timely manner, the child’s condition can only get worse. Over time, the bones will begin to become more deformed, causing pain and discomfort. In addition, untreated clubfoot leads to serious consequences:
- shortening of an abnormal limb;
- reduction in foot size;
- child's retardation in physical development;
- curvature of the spinal column;
- frequent ankle sprains;
- disability.
Causes of clubfoot
There is both congenital clubfoot and an acquired form of this disease. Therefore, the reasons may be different.
With congenital clubfoot, there can be three types of causes.
- Mechanical. Such reasons include too much pressure from the walls of the uterus on the fetus during pregnancy, in particular on its feet.
- The disease can also be inherited.
- The cause may also be neuromuscular. It manifests itself in the development of any pathologies in the baby during pregnancy.
If the disease has an acquired form, then the reasons for this may be the following.
- A sudden appearance of inflammation on the feet.
- Improper functioning of the nervous system.
- Burns around the feet.
- Incorrect growth of the leg bones.
- The presence of various tumor diseases.

Clubfoot in children under 12 months of age
☝ Special attention should be paid to this period. When a disease in an infant ⛹ has very pronounced signs, parents try to do everything possible to overcome this disease. When clubfoot was discovered only at an appointment with a medical specialist, fears arise for the health of your baby. Some doctors say that the baby will easily outgrow this problem and there is no need to worry. This is explained by the plasticity of the body at an early age.
However, we should not forget that even the slightest curvature of the foot can lead to improper development of the baby’s muscles.
Overloading one muscle and not enough tension in another can lead to a variety of consequences.
- Sleep disturbances.
- Headaches.
- Too slow both mental and physical development.
- Curvature of the legs.
- Rachiocampsis.
- A habit appears of placing your foot in the wrong way.
If clubfoot occurs in children under one year of age, you should immediately try to cure the disease.
Prevention
To prevent the development of clubfoot in a child, it is necessary to take a number of effective preventive measures:
- Pay a little attention to how the child walks. Children's footprints can tell a lot about the presence of abnormalities in the development of the ankle joint.
- Limit walking for a one-year-old child so as not to overtire his legs.
- Instill in your child an active lifestyle: morning exercises, cycling, games, swimming.
- Balance the children's diet. Include foods rich in microelements and minerals in your diet.
- Buy only high quality shoes for your child. It should have an instep support and a strong back.
- Periodically encourage the child to walk barefoot on an orthopedic mat, pebbles, or grass.
You shouldn’t turn a blind eye to the pathological changes you see in a child’s foot. The child simply needs full development: not only physical, but also mental. The assistance provided by a specialist will restore the damaged limb and enable the child to have a happy childhood.
Types of clubfoot
The International Classification of Diseases classifies clubfoot as a group of congenital foot deformities. Highlight:
- Equina varus clubfoot.
- Calcaneal-varus clubfoot.
- Calcaneal-valgus clubfoot.
According to the severity of clubfoot, it can be:
- Mild degree – changes are minimal. Completely curable with conservative methods.
- Moderate severity. Deformations of the foot are more pronounced, underdevelopment of muscles and ligaments is detected, and damage to the ankle joint is present.
- Severe degree. Significant pathological changes in the foot and ankle joint. Conservative treatment is ineffective.
- Very severe degree - cure is impossible. This degree leads to disability.
Treatment according to Komarovsky
Dr. Komarovsky says about clubfoot in children that treatment should begin as early as possible, even if the baby does not walk yet. The doctor recommends complex treatment, involving a combination of different methods.
Shoes
If a child is clubbed when walking, Komarovsky recommends wearing orthopedic shoes. Such shoes promote the correct placement of the foot and prevent it from moving.
Orthopedic shoes have an anatomical sole. On its inner side there are instep supports that prevent the foot from moving. Therapeutic shoes should have a small heel and a hard heel. You need to wear these shoes all the time.
Massage
The method is effective for mild to moderate disease. Massage helps eliminate muscle hypertonicity and helps give the foot the correct position. Massage treatment should only be performed by a specialist who knows the anatomical location of bones, muscles and ligaments in a child’s foot.
The therapeutic course of massage takes a long time - until the foot is completely straightened. It must be repeated periodically to prevent relapse. Massage for clubfoot in a child includes rubbing, kneading, twisting and stretching the foot.

Massage treatment according to Komarovsky
Gymnastics
Therapeutic exercises are recommended for any degree of clubfoot. Depending on the age of the child, the doctor selects exercises. Gymnastics is carried out in a playful way:
- Draw a straight line on the floor and invite the baby to walk along it so that the toe and heel are at the same level;
- Run across the room on your heels;
- Place the child on a chair, invite him to hold a felt-tip pen in his toes and draw a picture on a piece of paper;
- Place the baby on a chair, lay a towel on the floor in front of him, put a toy on one end of it - the child needs to drag the towel with the toy towards him with his toes;
- Invite your baby to goose step.
Gymnastics should be given 15-20 minutes daily. Exercises should not cause pain in the child. The child is barefoot during gymnastics classes. After finishing the session, it is recommended to take a warm foot bath.
Physiotherapy
Dr. Komarovsky considers physiotherapy to be one of the methods for treating a child’s clubfoot. They are done when the child is at least two years old and has a mild or moderate degree of pathology.
Useful ones are:
- Paraffin and ozokerite applications;
- Pine baths;
- Electrophoresis;
- Diadynamic currents.
Physiotherapy helps eliminate hypertonicity of the legs. Physiotherapy is carried out in courses of 10-15 procedures every six months.
Plastering
This method is used in cases of severe clubfoot in a child, when he can already walk. A plaster boot is put on the feet up to the middle of the shin, which rigidly fixes the foot in the correct position.
Interesting!
Today, the plaster casting method is being replaced by the use of special orthoses that can be removed at night.

Gymnastics, physiotherapy and plaster casting for clubfoot
Operation
For severe clubfoot, conservative methods are ineffective. The child can only be cured through surgery. The operation consists of eliminating bone deformities and suturing the ligamentous apparatus.
The postoperative period requires wearing orthoses, then orthopedic shoes. Massages and therapeutic exercises are also provided.
Children's clubfoot is easily corrected if treatment is started as early as possible. This is exactly what the famous pediatrician Komarovsky calls for. At the initial stage, the disease can be eliminated only with the help of orthopedic shoes, massage and gymnastics, if done regularly.
Causes and risk factors
The exact causes of the pathology have not yet been elucidated. Presumably, most often congenital clubfoot in children is caused by incorrect position of the fetus in the uterus or oligohydramnios. In addition, the formation of clubfoot in children can be influenced by the alcohol, drug and tobacco addiction of a pregnant woman, as well as genetic factors that contribute to disturbances in the formation of the musculo-ligamentous apparatus at the prenatal stage of development, deficiency of nerve fibers, muscle underdevelopment, etc.
Acquired clubfoot in children can develop due to wearing unsuitable shoes, muscle paralysis, poliomyelitis, underdevelopment of bones, previous leg diseases, traumatic injuries of the lower extremities (ligaments, bones), burns of the feet, rickets, due to increased load on the feet with increased growth and child weight gain.
The typical form of clubfoot in children develops against the background of a disorder in the structure of ligaments, tendons and muscles. The atypical form of clubfoot can be caused by diseases of the central nervous system, as well as serious disorders of the musculoskeletal system.
Forms of the disease
Clubfoot in children is divided into congenital and acquired.
It is recommended to correct the congenital form of clubfoot in children during the first months of the child’s life (optimally up to 4 months), otherwise the pathology will worsen.
Depending on the involvement of the limbs, clubfoot in children can be unilateral or bilateral.
There are two main forms:
- typical clubfoot;
- atypical clubfoot.
Depending on the severity of the disease, three degrees of the typical form of the disease are distinguished:
- varus contractures (I degree) – have a mild course and are amenable to manual correction;
- soft tissue form (II degree) – characterized by the inability to completely place the foot on the floor. There is resistance from soft tissues during manual correction of the defect;
- bone form (III degree) – is relatively rare and is characterized by severe deformation of the foot due to pathology of bone and soft tissues; it cannot be treated conservatively.
Clinical and etiological classification of clubfoot:
- idiopathic – reduction of the talus, equinus, violation of the relative position of the front and back of the feet, shortening of the calf muscle, disorders of the joints of the foot, pathology of the blood vessels of the anterior parts of the leg;
- postural, or positional - the talus and calcaneus are unchanged, the articular surfaces are developed normally, but are in a state of subluxation;
- congenital clubfoot in combination with congenital myo- and neuropathy - secondary deformation of the foot caused by developmental disorders of other parts of the musculoskeletal system (for example, congenital dislocation of the hip);
- syndromological - combines congenital clubfoot, combined with congenital myo- and neuropathy with developmental anomalies of other organs.










